
How Retinol Works: The Cell Renewal Science Explained
Published June 5, 2026 · Updated July 12, 2026

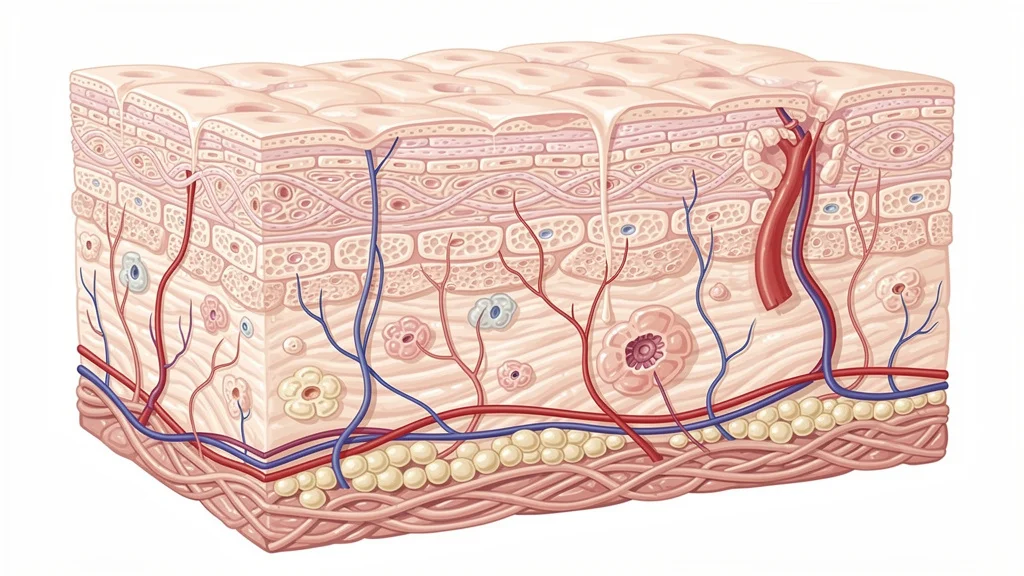
Retinol triggers a cascade of cellular events that speed up skin renewal and strengthen the dermis. When applied topically, the fatty molecule penetrates the stratum corneum, where enzymes convert it into the active metabolite retinoic acid. That small compound enters skin cell nuclei and binds directly to retinoic acid receptors (RARs) and retinoid X receptors (RXRs) — proteins that switch on genes controlling division, differentiation, and collagen production. Within days, the epidermis begins shedding old layers more efficiently, while fibroblasts ramp up synthesis of new collagen and elastin. The result is visibly smoother texture, faded discoloration, and firmer skin over time.
What Exactly Is Retinol and How Does It Differ from Retinoids?
Retinol belongs to the broader family of retinoids, which are all vitamin A derivatives. Prescription-strength retinoids — such as tretinoin (all‑trans retinoic acid) — are already in the active acid form and bind receptors immediately. Over‑the‑counter retinol, in contrast, must first undergo two enzymatic oxidation steps inside the skin to form retinaldehyde and then retinoic acid. This built‑in metabolic bottleneck makes retinol orders of magnitude gentler than tretinoin, while still delivering similar long‑term anti‑aging benefits. Because the conversion is rate‑limited, less free retinoic acid is available at any given moment, which reduces the risk of redness and peeling while still training the skin to renew itself.
Retinyl esters (retinyl palmitate, retinyl propionate) sit one step further back in the conversion pathway and are even milder, making them common in entry‑level formulations. Hydroxypinacolone retinoate (HPR), a newer retinoid ester, binds RARs directly without the need for metabolic activation, offering a unique balance of efficacy and tolerability. This gradation in strength explains why a retinol serum can bridge the gap between drugstore creams and dermatologist‑prescribed treatments.
How Does Retinol Trigger Cell Renewal at the Molecular Level?
Once retinoic acid enters the nucleus of a basal keratinocyte, it forms a heterodimer complex with RAR and RXR. This complex latches onto specific DNA sequences called retinoic acid response elements (RAREs), located in the promoter regions of more than 500 genes. The resulting transcription changes accelerate the mitosis of keratinocytes in the basal layer, push younger cells upward faster, and suppress the production of irregular, sticky keratin that contributes to rough texture.
At the same time, retinoic acid down‑regulates collagen‑degrading matrix metalloproteinases (MMPs) — especially MMP‑1, MMP‑3, and MMP‑9 — that sunlight and aging chronically activate. The net effect is a thicker, more compact epidermis and a denser dermal matrix. This dual action explains why fine lines, sun spots, and laxity gradually improve: old, damaged cells are shed more rapidly, while fresh, organized tissue replaces them.
From Retinol to Retinoic Acid: The Conversion Pathway
When you smooth a retinol serum onto your face, the molecule encounters two key enzyme families: alcohol dehydrogenases (ADHs) and aldehyde dehydrogenases (ALDHs). ADH first oxidizes retinol into retinaldehyde, then ALDH converts retinaldehyde into all‑trans retinoic acid. This two‑step reaction occurs predominantly inside keratinocytes and sebocytes, which naturally stock these enzymes. The process is self‑limiting because the skin’s enzyme capacity maxes out — a built‑in safety valve that protects against retinoic acid overload.
The transformation also depends heavily on cellular retinoic acid‑binding proteins (CRABPs), which shuttle freshly made retinoic acid to the nucleus. CRABP‑2, in particular, shepherds the molecule to RARs while protecting it from premature catabolism by cytochrome P450 enzymes. Any disruption in this delivery system — from oxidative stress, UV damage, or simply age‑related enzyme decline — can reduce the amount of functional retinoic acid a cell receives. That’s why formulations that stabilize retinol and support the skin’s natural enzyme activity tend to deliver more predictable results after eight to twelve weeks of consistent use.
How Does Retinol Remodel Collagen and Elastin?

In the dermis, fibroblasts respond to retinoic acid by up‑regulating the genes COL1A1 and COL3A1, which code for the alpha chains of type‑I and type‑III collagen. At the same time, tissue inhibitor of metalloproteinase‑1 (TIMP‑1) expression rises, neutralizing the collagen‑chopping MMPs. The net result is a measurable increase in procollagen production within the papillary dermis — the uppermost layer that gives skin its bounce.
This collagen rebuilding process is slow, because a single fibroblast cycle takes several weeks. Clinically, the first visible improvement often appears around week 8, with meaningful dermal thickening documented by ultrasound after 12 to 24 weeks of regular use. Elastin fibers also benefit: retinoic acid helps reorient fragmented elastic fiber networks into a more organized, functional scaffold, which visibly reduces crepiness around the eyes and jawline.
Why Does Retinol Sometimes Cause Irritation?
The “retinoid reaction” — redness, flaking, and heightened sensitivity — results from a temporary surge in epidermal turnover and a weakening of the skin barrier. As keratinocytes proliferate and migrate faster, the stratum corneum thins transiently, increasing transepidermal water loss. Simultaneously, retinoic acid activates TRPV1 receptors, the same heat‑and‑pain sensors that respond to capsaicin, lowering the threshold for stinging and warmth.
This adjustment phase, called retinization, typically lasts two to four weeks. The skin adapts by up‑regulating barrier lipids — ceramides, cholesterol, and fatty acids — and by thickening the stratum granulosum. For people living in the high‑UV regions of the American South and West, where daily sun exposure already stresses the barrier, pacing retinol introduction is especially critical. Using a pea‑sized amount every third night, buffering with moisturizer, and applying next‑generation retinoids that bypass the conversion bottleneck can dramatically shorten the uncomfortable window.
How Can You Fit Retinol Into a Real‑Life Skincare Routine?
Start with a low concentration (0.1% to 0.3% retinol or an HPR‑based formula) applied only in the evening. Cleanse, pat skin completely dry, then disperse a pea‑sized drop over the entire face, avoiding the eye hollow and mouth corners. After five minutes, layer a fragrance‑free moisturizer to seal in hydration. Morning after, wash with a gentle cleanser and apply a broad‑spectrum sunscreen with SPF 30 or higher — non‑negotiable because retinoic acid thins the stratum corneum and makes skin more vulnerable to UV‑induced DNA damage.
Gradually increase frequency from twice a week to every other night over three weeks. If stinging persists, back off to every third night and buffer the serum under moisturizer. Once your skin tolerates nightly application, you can consider stepping up to a more potent complex that includes complementary ingredients like peptides — an approach that lets you maintain progress without overtaxing your barrier. Products that pair HPR with matrix‑supporting peptides, such as the ageLOC Tru Face Peptide Retinol Complex, are designed to deliver retinoic acid‑like signaling while calming the surrounding tissue, a helpful option for those navigating intense summer UV or drier climates.
Does Retinol Actually Improve Hyperpigmentation and Acne?
Yes, through three parallel mechanisms. First, accelerated corneocyte shedding physically removes melanin‑loaded cells from the epidermis, reducing dark spots. Second, retinoic acid suppresses tyrosinase transcription, the key enzyme in melanin synthesis, so new spots are less likely to form. Third, in acne‑prone skin, retinol normalizes desquamation inside the follicle, dislodging the microcomedones before they become inflamed papules.
Because of these overlapping benefits, dermatologists often recommend an over‑the‑counter retinol as a first step before considering prescription retinoids for persistent post‑acne marks or melasma. For the 40% of U.S. adults who report some degree of hyperpigmentation according to a 2022 American Academy of Dermatology survey, a well‑formulated retinol can be a cornerstone of a multi‑pronged brightening regimen that also includes vitamin C during the day and niacinamide at night.
What Makes HPR a Unique Retinoid?
Hydroxypinacolone retinoate (HPR) is an ester of all‑trans retinoic acid engineered to bind RARs directly, without the enzymatic conversion steps that limit retinol’s speed and predictability. Because it arrives at the receptor pre‑activated, HPR delivers retinoic acid‑like gene expression at significantly lower doses, which translates into less barrier disruption. In a 2016 in‑vitro study published in the Journal of the American Academy of Dermatology, HPR was found to regulate RAR‑gamma — the subtype most prevalent in skin — at nanomolar concentrations comparable to tretinoin, yet with a markedly lower pro‑inflammatory cytokine release.
This direct‑action mechanism makes HPR especially appealing for those who have struggled with traditional retinol or who live in high‑exposure climates such as Arizona, Texas, or Florida, where sun‑weakened skin can’t afford a long, irritated adjustment period. When combined with signal peptides that tell fibroblasts to produce more collagen and elastin, HPR-based formulations enable a nightly routine that stays on the right side of comfortable while still driving measurable anti‑aging change.
How Does Sun Exposure Interact With Retinol‑Treated Skin?
Retinyl esters and retinoic acid themselves are photolabile — they degrade when UV light hits them, generating free radicals that can damage DNA. At the same time, the thinner, renewing stratum corneum offers less natural sun scatter. For someone in Los Angeles or Phoenix who is exposed to UV indexes of 8 and above for much of the year, using retinol without rigorous sun protection can undermine the very progress it creates.
Application timing solves most of these concerns. Retinol products should be part of the nighttime routine, applied on clean skin, and washed off in the morning. During the day, a mineral or hybrid sunscreen with SPF 50 and high UVA protection is essential. Choosing a gentle retinol alternative that contains photostable ingredients can also mitigate the small amount of residual retinoid that might remain in the stratum corneum even after washing, further easing the risk for outdoor‑active people.
Frequently Asked Questions
Can I use retinol every night from the start?
No. Begin twice a week and increase slowly. Daily application too soon can overwhelm the retinization process and cause prolonged redness, peeling, and barrier damage.
Is retinol safe during pregnancy or breastfeeding?
Oral retinoids are known teratogens, and while topical retinol absorption is minimal, most obstetricians and the American College of Obstetricians and Gynecologists advise discontinuing all retinoids during pregnancy and nursing out of an abundance of caution.
How long until I see visible anti‑aging results from retinol?
Smoother skin texture may appear in 4–6 weeks. Significant reduction of fine lines and pigmentation usually takes 8–12 weeks. Collagen remodeling visible under ultrasound requires at least 3–6 months of consistent use.
Can I layer retinol with vitamin C or other exfoliants?
Vitamin C (L‑ascorbic acid) works at a low pH, while retinol prefers a more neutral environment. Using them together may irritate skin. Better to split the routine: vitamin C in the morning, retinol at night. Avoid combining retinol with alpha‑hydroxy acids or benzoyl peroxide in the same session unless a product is specifically formulated for that purpose.
What percentage of retinol should a beginner choose?
Start with 0.1%–0.3% retinol or an HPR‑based formula, which tends to be less irritating. Prescription‑strength tretinoin usually starts at 0.025%, but over‑the‑counter options allow more gradual adaptation.
Does retinol thin the skin over time?
No. Retinol initially thins the outer dead‑cell layer (stratum corneum) but thickens the living epidermis and dermis over months. Histological studies confirm increased epidermal thickness and denser collagen after long‑term retinoid use.
NuBest Skin is an Independent Nu Skin Brand Affiliate -- not produced or endorsed by Nu Skin Enterprises Inc.