
How Retinol Actually Works on Your Skin: The Science of Renewal
Published 5 June 2026 · Updated 12 July 2026

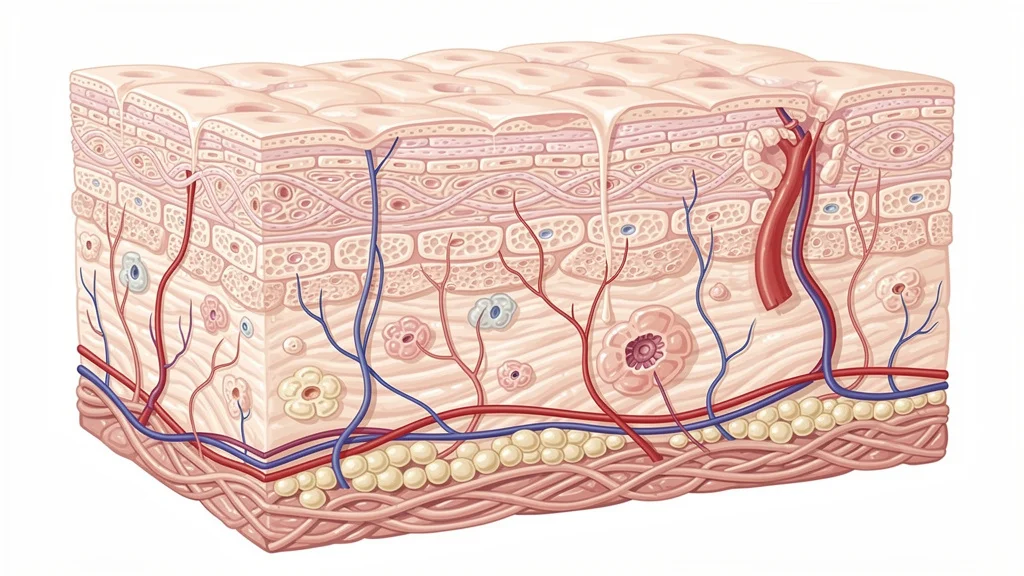
Retinol doesn’t just “speed up” skin renewal—it rewires the genetic programme inside your cells. When you apply a retinol cream, the molecule travels into the living epidermis and undergoes a two‑step enzyme conversion to become all‑trans retinoic acid, the active form of vitamin A. That active metabolite binds to retinoic acid receptors (RAR‑α, RAR‑β, RAR‑γ) in the nuclei of keratinocytes and fibroblasts. The receptor‑ligand complex then switches on genes that increase epidermal turnover, boost glycosaminoglycan synthesis, and suppress collagen‑destroying matrix metalloproteinases (MMPs) in the dermis. Within about four weeks of nightly use, desquamation rates rise and fine lines begin to soften because the skin is literally rebuilding itself from the inside out. This is the same fundamental pathway that prescription tretinoin uses—retinol is simply a gentler, time‑released precursor.
What is retinol, and how is it different from a retinoid?
Retinol is one member of the retinoid family—all molecules derived from vitamin A. In over‑the‑counter skincare, “retinoid” covers everything from retinol esters (retinyl palmitate) to retinaldehyde and retinol itself. Prescription retinoids like tretinoin and adapalene are already in their active acid form, so they work faster but are more irritating. Retinol sits in the middle: it must be enzymatically converted first to retinaldehyde, then to all‑trans retinoic acid, inside the skin. This two‑step metabolism creates a built‑in buffer that makes retinol up to 20 times less irritating than tretinoin, while still delivering measurable anti‑ageing benefits. That characteristic is especially useful in Ireland’s mild, damp climate where central heating and sudden humidity shifts can already weaken the skin barrier, making aggressive acids a challenge for sensitive cheeks.
Why does retinol need to be converted inside the skin?
Retinol is a pro‑drug. It cannot bind retinoic acid receptors until it is oxidised to all‑trans retinoic acid. Freshly applied retinol diffuses through the stratum corneum and into viable keratinocytes, where alcohol dehydrogenase (ADH) enzymes transform it into retinaldehyde. A second enzyme, retinaldehyde dehydrogenase (RALDH), completes the oxidation to retinoic acid. The rate of conversion depends on the skin’s own enzyme supply, which varies from person to person and drops with age. That’s why the same 0.5% retinol serum can feel too weak for one person and too aggressive for another. On a damp Galway morning, when the barrier is slightly hydrated, retinol penetration may be faster; on a cold, wind‑chapped day, it can be slower. This variable conversion is the main reason chemists have developed direct‑acting retinoid esters that bypass the two‑step pathway.
How do retinoid receptors actually trigger cell renewal?
Once all‑trans retinoic acid enters the nucleus, it forms a heterodimer with retinoid X receptors (RXRs) and latches onto specific DNA sequences called retinoic acid response elements (RAREs). This complex behaves like a dimmer switch: it can upregulate genes that promote epidermal proliferation and differentiation, while simultaneously downregulating MMPs—enzymes that degrade collagen fibres after UV exposure. The net result is a thicker epidermis, a more compact stratum corneum, and a dermis with denser, better‑organised collagen bundles. A 2016 randomised controlled trial published in the Journal of Investigative Dermatology found that retinoic acid reduced MMP‑1 (collagenase) by approximately 80% in photodamaged skin after four months of daily use. While retinol’s effect is milder, it triggers exactly the same receptor‑mediated cascade.
What is the role of cell turnover in anti‑ageing?

Young skin replaces its outermost corneocytes roughly every 28 days. By age 60, that cycle can stretch to 45 days or more. Slower turnover causes dead cells to sit on the surface, scattering light and creating a sallow, tired look. Retinoids re‑accelerate this biological clock. They boost the expression of KRT6 and KRT16 keratins—markers of rapid proliferation—so new cells push upwards more quickly. At the same time, retinoic acid stimulates the production of epidermal hyaluronic acid, which holds water and gives skin that plump, “glowing” appearance often noticed after a few weeks of consistent retinol use. In Irish weather, where overcast skies can make skin look dull even in summer, this glow‑restoring mechanism is one of the most immediately visible retinol effects.
Exfoliation versus true renewal
It’s easy to confuse turnover with exfoliation, but they are not the same. AHA scrubs dissolve the glue between dead cells; retinoids change the rate at which new cells are born. This deeper action explains why retinol results take 8–12 weeks, but the improvements—smaller pore appearance, smoother texture, less creepiness around the eyes—tend to be cumulative and lasting.
How do retinoids boost collagen in the dermis?
The dermis is where the real anti‑ageing battle takes place. Fibroblasts that once pumped out type I collagen slow down with age, while UV‑activated MMPs chew through existing fibres. All‑trans retinoic acid lowers MMP‑1, MMP‑3, and MMP‑9 levels while upregulating tissue inhibitors of metalloproteinases (TIMPs) and directly stimulating the COL1A1 and COL1A2 genes. A histological study of forearm skin treated with 0.1% tretinoin for 12 months showed a 40% increase in new collagen formation in the papillary dermis. Retinol studies, though less dramatic, still report significant collagen density improvements at 0.3%–1% concentrations over 24 weeks. Because Ireland’s UV index stays low for much of the year, collagen preservation is an achievable long‑term strategy—fewer incidental UV rays means less MMP activity to counteract the retinoid’s repair signals.
Why do modern formulations use retinoid esters like HPR?
Hydroxypinacolone retinoate (HPR) is a retinoic acid ester that binds RAR‑γ and RAR‑α directly, without needing any enzymatic conversion. This first‑pass freedom gives HPR the activity of a prescription retinoid with a fraction of the irritation. Because the molecule is already in an ester form, it’s also more stable in air and light—a genuine advantage when you’re opening a bottle in a steamy bathroom after an Irish shower. Independent clinical testing has shown that 0.2% HPR can reduce fine lines as effectively as 0.5% retinol, with less stinging and peeling. The ageloc Tru Face Peptide Retinol Complex pairs HPR with signal peptides to amplify the collagen‑boosting cascade, creating a formula designed for skin that needs consistent age‑repair without the classic retinoid “ugly” phase.
What concentration of retinol actually works—and how fast?
Efficacy starts around 0.01% but really becomes noticeable in clinical photographs at 0.05%–0.1%. Most high‑street products in Ireland, from brands like The Ordinary or CeraVe, land between 0.2% and 1%. Lower strengths (0.2%–0.3%) are ideal for beginners because they still trigger receptor activity while keeping barrier disruption minimal. At 1%, results appear faster but redness and flaking become much more likely, especially in rooms heated by radiators that already pull moisture from the air. A twelve‑week split‑face study demonstrated that 0.3% retinol improved periorbital wrinkles by 23% on average, with side‑effect rates half those of a 1% formula. The key is frequency: nightly use is more effective than occasional “shock” treatments, no matter the percentage.
How can Irish skin types get the best from a retinoid routine?
Mild, damp, low‑UV conditions are actually kind to retinol users—there’s less incidental sun damage to undo, and the humidity helps keep the barrier hydrated. Still, a good routine matters. Apply a pea‑sized amount to dry skin (water increases penetration and irritation), wait ten minutes, then seal with a ceramide‑rich moisturiser. On nights when windburn has left cheeks tight, skip the retinoid or use a gentler HPR ester. Always wear SPF 30 or higher during the day, even in winter, because retinoic acid thins the compacted stratum corneum and makes skin more photosensitive. And don’t layer acidic toners or vitamin C at the same time—separate them into morning and evening slots to avoid over‑activation of irritant receptors. With these simple habits, a retinoid becomes a long‑term companion, not a weekend project, and delivers the kind of calm, resilient skin that looks healthy under a soft Irish drizzle.
Here are direct, science‑backed answers to the questions people really search for about retinol and vitamin A skincare.
Frequently Asked Questions
Does retinol thin the skin over time?
No, clinical biopsies show the opposite. Retinoids thin the outer, compacted dead‑cell layer (stratum corneum) while thickening the living epidermis and dermis beneath. This dual action improves texture and reduces fine lines without weakening the skin’s structural integrity. The temporary “thin” feeling is actually a smoother, better‑hydrated surface.
Can I use retinol around my eyes?
Yes, but the periorbital skin is thinner and more permeable, so a lower concentration (0.1%–0.2% retinol or an ester like HPR) and a buffering eye cream are recommended. Apply it to the orbital bone, not the mobile eyelid, and always protect the area with SPF during the day because increased cell turnover makes the skin more UV‑sensitive.
Why does my skin get worse before it gets better on retinol?
The early ‘retinoid purge’ happens because accelerated cell turnover pushes pre‑existing microcomedones—tiny clogged pores that were already forming—to the surface all at once. It usually lasts four to six weeks. If breakouts continue beyond eight weeks, the product may be too occlusive or contain other comedogenic ingredients rather than the retinoid itself.
Is retinol safe to use during pregnancy?
While topical retinol has not been proven to cause birth defects in the way oral isotretinoin does, the HPRA and the Irish Medicines Board advise avoiding all vitamin A derivatives during pregnancy and breastfeeding as a precaution. Always consult your GP or midwife before continuing any retinoid product.
Does retinol expire or lose potency?
Yes. Retinol is sensitive to light, heat, and oxygen. An opened bottle typically retains full potency for three to six months if stored in a cool, dark cabinet. Pump dispensers protect the formula better than jars. If the product turns yellow‑orange or smells rancid, the retinol has oxidised and lost effectiveness.
How long until I see real changes from retinol?
Initial glow and smoother texture often appear after 4–6 weeks of consistent nightly use. Fine‑line reduction and firmer skin become visible around 8–12 weeks. Deeper collagen remodelling continues for 6–12 months, so the best results accumulate with long‑term, uninterrupted use.
NuBest Skin is an Independent Nu Skin Brand Affiliate -- not produced or endorsed by Nu Skin Enterprises Inc.